A superbill is a detailed medical document. It is provided by your healthcare provider. Your medical superbill includes the services you received, along with the required medical codes used for insurance reimbursement. If you are paying for healthcare services out of pocket—… specially when visiting your out-of-network provider, you can use your therapy or medical superbill to submit a claim to your insurance company and recover eligible costs.
In simple terms, a superbill acts as both a record of your medical visit and a structured document that helps your insurance provider understand what treatment was given and how much reimbursement you may receive.
Understanding how superbills work not only helps you manage your healthcare expenses more effectively but also ensures you don’t miss out on reimbursements you may be entitled to.
What Is a Superbill in Medical Billing?

With the number of documents attached to a single medical visit, it might make the patient swear off it forever. From diagnosis codes to insurance claims and reimbursements, both patients and healthcare providers are bound to feel confused by medical billing at one point. Regardless, each document plays a crucial role in ensuring that healthcare services are properly recorded and paid for. Among those is the superbill.
A superbill is a comprehensive document provided by healthcare staff to the patient. It includes detailed information about their visit, which is later used to create an insurance claim.
Your simple medical bill is different because a superbill contains important medical coding information to make it easier for insurance companies to understand the treatment provided and evaluate how much reimbursement you may receive. It documents the diagnosis, procedures performed, and charges associated with the services provided.
In simple terms, a superbill comprises of a medical receipt and billing codes that help insurers in processing a claim.
What are the Types of Superbills?
There are multiple forms of superbills depending on the healthcare practice and the type of services provided. Many providers customize their superbills to match their specialty.
Here are some common types:
1. Standard Superbills
Standard superbills are rendered for routine medical visits and general healthcare services. They usually contain common diagnoses and procedures that are frequently performed in the practice.
2. Specialty-Specific Superbills
Certain healthcare providers with specialties may use customized superbills tailored to their field. For example, dermatology, psychiatry, or physical therapy superbills might differ from one another based on procedure and diagnosis codes specific to those services.
3. Electronic Superbills
With the rise in digital tools, many practices now rely on generating superbills via electronic health record (EHR) systems.
The Importance of a Superbill in Medical Billing!
Superbills have an important role in the medical billing process. Because they contain the core information needed to create and verify insurance claims.
For healthcare providers, the document helps ensure that services are accurately documented and coded. Meanwhile, for patients, superbills serve as a structured document that can be submitted to insurance companies when seeking reimbursement for out-of-pocket expenses.
Overall, superbills help:
- Maintain accurate billing records.
- Support proper medical coding.
- Reduce claim errors.
- Provide documentation for insurance reimbursement.
Components of a Superbill
A superbill contains several important elements that allow insurance companies to review and process reimbursement requests from patients.
Patient Information
This section includes the patient’s name, date of birth, and contact details.
Provider Information
The healthcare provider’s name, practice information, and National Provider Identifier (NPI) are included so insurers can verify the provider.
Visit Information
This section lists the date of service and the type of medical visit or consultation.
Medical Codes
Superbills include diagnosis codes and procedure codes that describe the condition treated and the services performed.
Charges for Services
The cost associated with each medical service provided during the visit is listed.
Provider Signature
Some superbills require the provider’s signature to confirm that the information is accurate.
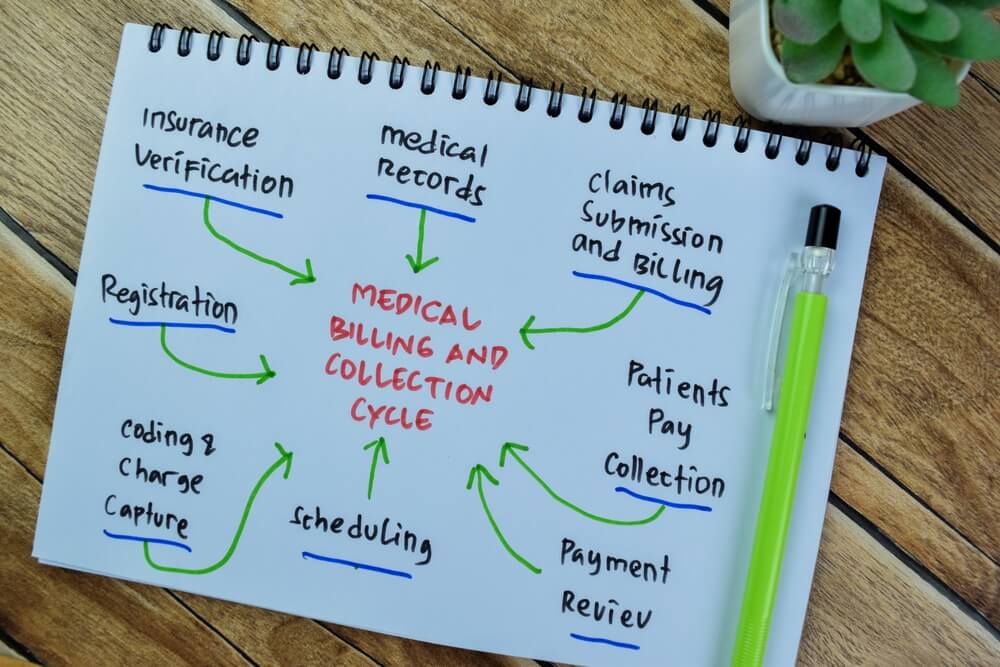
How Does a Superbill Work?

The process of using a superbill is relatively straightforward. It starts from utilizing a healthcare service and ends with the submission of an insurance claim by the patient.
A healthcare provider documents the treatment rendered to the patient, which helps in generating a superbill containing information about the diagnoses, procedures, and associated costs.
Superbills are usually applicable to those patients who have paid for the service out of pocket. The insurance provider reviews the superbill to determine whether the services are eligible for reimbursement under the patient’s policy.
Once approved, the insurance company reimburses the patients for the covered portion of the medical expenses.
Superbills reimbursement is especially common when patients visit out-of-network providers, such as private practices, mental health clinics, and specialty healthcare services that do not directly bill their insurance plan.
Who Uses Superbills?
Superbills in healthcare are used by several parties within the system, including providers, patients, and even medical billing professionals.
Physicians, therapists, and psychologists often prepare therapy superbills to document patient visits and support billing processes.
Patients use a superbill for insurance reimbursement when they have paid out of pocket for healthcare services.
Billing teams may use superbills as a reference when preparing insurance claims and ensuring proper coding.
Superbill vs Receipt vs Statement: What’s the Difference?
An influx of billing documents following a medical visit is bound to confuse a patient. Thus, it is important to distinguish between them as they serve different purposes in healthcare billing.
A superbill is essentially a detailed document containing medical codes, service descriptions, and provider information used for insurance reimbursement.
A receipt is simply proof that a payment was made. It usually contains the amount paid without details about medical codes or diagnoses.
A billing statement is prepared by an insurance company containing information about the balance owed to the patients after insurance payments have been applied.
What are the Benefits of Superbills for Patients?

Superbills have a great many benefits to patients who need to manage healthcare expenses and insurance reimbursements.
As the medical expenses are comprehensively outlined in the bill, it helps in easier verification of claims once they are submitted to the insurer.
It also promotes transparency between the healthcare provider and the patient regarding the charges associated with the services provided.
Patients can also track their medical expenses via superbills for tax purposes or reimbursement through health savings accounts (HSAs).
Common Mistakes to Avoid with Superbills!

Errors in superbills can lead to claim rejections or delays in reimbursement. Therefore, healthcare providers and billing teams should carefully review superbills before issuing them to ensure that all necessary details are included.
Some common mistakes include:
- Missing patient or provider information.
- Incorrect diagnosis or procedure codes.
- Incomplete service descriptions.
- Missing provider identification numbers.
- Poorly formatted or illegible documentation.
Common Superbill Errors That Can Delay Reimbursement!
Insurance companies rely on accurate coding and documentation to effectively process claims. Even small errors can cause claims to be rejected or require resubmission, resulting in slower reimbursement. These include:
- Incorrect diagnosis codes.
- Incorrect procedure codes.
- Mismatched service dates.
- Missing provider details.
- Missing signatures.
When Should Patients Request a Superbill?
Patients can request a superbill whenever they need documentation to submit an insurance claim for reimbursement.
This typically happens when:
- Visiting an out-of-network healthcare provider.
- Paying for services out of pocket.
- Submitting claims directly to insurance companies.
- Filing reimbursement requests through health savings accounts or employer health programs.
Superbills in medical billing ensure patients have the proper documentation needed to recover eligible healthcare expenses from their insurance provider.
FAQs
Who prepares a superbill?
A superbill is prepared by the healthcare provider featuring an outline of the services provided to a patient visit.
Is a superbill the same as an invoice?
No, a superbill is not the same as an invoice, as the former includes medical billing codes and clinical details required for insurance reimbursement. Meanwhile, an invoice is simply the list of services and their associated charges.
Can patients submit superbills to insurance companies?
Yes, superbills are typically sent to insurance companies by the patients after they have paid out of pocket for a healthcare service utilized.
What codes are included in a superbill?
A superbill comprises of diagnosis codes (ICD) and procedure codes (CPT or HCPCS) that describe the patient’s condition and the services performed.
What happens if my insurance company denies my superbill?
If a superbill is denied, the patient may need to review the reason for denial, correct any errors, or contact the insurance provider to appeal the decision.